Drug name
Last update: May 2026Lenacapavir Once-Yearly
Developer(s)
Drug information
Lenacapavir Once-Yearly
Investigational
Small molecule
Capsid inhibitor
Once yearly lenacapavir (LEN) is an investigational intramuscular injectable formulation currently in clinical development for potential once-yearly HIV pre-exposure prophylaxis (PrEP). A phase I trial evaluating two once-yearly formulations found that a single 5000 mg intramuscular dose of lenacapavir resulted in sustained median plasma concentrations above those of the twice-yearly subcutaneous formulation (927 mg) for at least 56 weeks. Notably, the median concentrations at weeks 52 and 56 for the intramuscular formulations (50.7-65.6 ng/mL) were higher than the median concentration at week 26 (23.4 ng/mL) observed in PURPOSE 1 and 2. Once-yearly intramuscular lenacapavir may therefore further improve PrEP adherence, persistence, and scalability by offering reduced dosing frequency.
Formulation is currently in clinical development and not yet approved in any jurisdiction. The direct progression to phase 3 for once‑yearly IM lenacapavir is justified scientifically and accepted by regulators because phase 1 data showed plasma exposures (and safety) that matched or exceeded the pivotal efficacy PK thresholds for the approved twice‑yearly SC regimen. Annual IM depot’s PK tail and implementation differences, unaddressed by PK bridging alone, will require real-world post-marketing/surveillance.
Formulation is currently in clinical development and not yet approved in any jurisdiction. Once-yearly intramuscular LEN maintained plasma concentrations higher than those associated with efficacy for twice-yearly subcutaneous LEN for PrEP for >12 months (plasma exposures at one year exceeded levels associated with protection in PURPOSE trials). Both yearly investigational formulations were safe and tolerable. Results from phase 1 support moving to Phase 3 study for once-yearly IM LEN for HIV PrEP. WHO guideline refers to offering long‑acting injectable PrEP options as part of combination approaches, explicitly accepting PK/efficacy bridging for schedule changes and new depot products, provided safety and concentration requirements are met.
Therapeutic area(s)
- HIV
- Pre-Exposure Prophylaxis (PrEP)
- Prevention
Administration route
Intramuscular
Associated long-acting platforms
Aqueous Solution
Use of drug
- Administered by a community health worker
- Administered by a nurse
- Administered by a specialty health worker
- To be determined
- Yearly
to be determined
Dosage
3000 mg - 2x3mL intramuscular injections
5000 mg - 2x5mL intramuscular injections
Oral LEN 600 mg on Day 1 (with the IM injections) and Day 2 (The once‑yearly modality uses two investigational intramuscular (IM) formulations, distinct from the subcutaneous (SC) formulation used for twice‑yearly dosing)
Once-yearly intramuscular lenacapavir (5000 mg) provided higher Ctrough levels than the twice-yearly subcutaneous formulation. Future development suggests a lower optimal dose for the intramuscular option. A significant difference in the Phase I trial was the absence of oral loading doses for the once-yearly intramuscular formulation, which were required for the twice-yearly subcutaneous version due to its slow initial release. The intramuscular formulation also exhibited a faster initial increase in lenacapavir blood plasma concentration.
Not provided
Comment & Information
Developer(s)

Gilead Sciences, Inc.
Gilead Sciences, Inc. is a multinational biopharmaceutical company that develops and manufactures innovative medicines for life-threatening diseases, including anti-viral therapeutics for HIV/AIDS, Hepatitis B, Hepatitis C and Covid-19. Headquartered in Foster City, California, Gilead was originally founded in 1987 and is currently listed on both the S&P 500 and the NASDAQ Biotechnology Index.
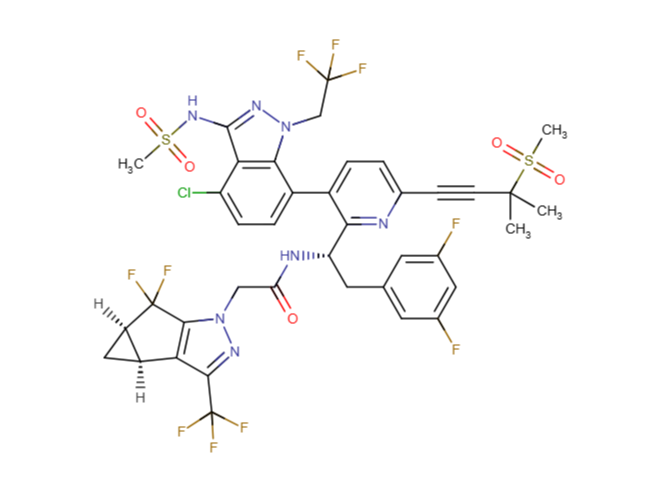
Drug structure
Scale-up and manufacturing prospects
LEN is already being manufactured at scale by Gilead for the twice-yearly SC product. For yearly IM, similar industrial processes will form the basis but with adaptations to the higher concentration and altered vehicle (ethanol content for IM depot). Equipment for injectable: Stainless steel pharmaceutical reactors, glass-lined reactors, rotary evaporator (rotovap), flash chromatography columns, stainless steel autoclave, cooling bath, silica gel chromatography columns, vacuum distillation apparatus, simulated moving bed chromatography system, Chiralpak columns.
Storage of injectable lenacapavir in borosilicate vials is contraindicated due to issues with chemical compatibility. Instead, it is recommended that vials are made from aluminosilicate glass. High-precision mixing tanks with capability for viscous, ethanol-containing solutions. Aseptic filling/isolation units compatible with ethanol/PEG vehicles.Sterile filtration units for low-volume injectables.Standard lyophilisation (if relevant to final formulation.
Vehicles with ethanol (often 5% or 10%) require specialised mixing times and solvent management to control viscosity and precipitation, which impact overall plant throughput and quality assurance. PEG and ethanol vehicles restrict direct steam sterilisation due to oxidation risk; sterile filtration is therefore preferred for terminal sterilisation—requiring high-quality, compatible filter assemblies with low extractable profiles.
Proton nuclear magnetic resonance (1H NMR), High-performance liquid chromatography (HPLC), Ultra-Performance Liquid Chromatography (UPLC). Container closure integrity testers (for glass vials or prefilled syringes). Stability chambers for long-term and accelerated conditions.
Excipients
Not provided
Not provided
Not provided
Delivery device(s)
No delivery device
Publications
Background
Long-acting antiretrovirals can address barriers to HIV pre-exposure prophylaxis (PrEP), such as stigma and adherence. In two phase 3 trials, twice-yearly subcutaneous lenacapavir was safe and highly efficacious for PrEP in diverse populations. Furthering long-acting PrEP efforts, this study assessed the pharmacokinetics and safety of two once-yearly intramuscular lenacapavir formulations.
Methods
This phase 1, open-label study in participants aged 18–55 years without HIV evaluated the pharmacokinetics, safety, and tolerability of two lenacapavir free acid formulations administered by ventrogluteal intramuscular injection as a single 5000 mg dose (formulation 1 with 5% w/w ethanol, formulation 2 with 10% w/w ethanol). Pharmacokinetic samples were collected at prespecified timepoints up to 56 weeks. Lenacapavir plasma concentrations were measured with a validated liquid chromatography–tandem mass spectrometry method and summarised with non-compartmental analysis. Pharmacokinetic parameters evaluated included the area under the concentration–time curve for the once-yearly dosing interval calculated from days 1 to 365 (AUCdays 1–365), peak plasma concentration, time to reach peak plasma concentration, and trough concentration (Ctrough). Plasma concentration data from phase 3 studies of twice-yearly subcutaneous lenacapavir (PURPOSE 1 and PURPOSE 2) were pooled for comparison with once-yearly intramuscular lenacapavir formulations. Safety and tolerability, including participant-reported pain scores, were assessed.
Findings
20 participants received lenacapavir formulation 1 and 20 received lenacapavir formulation 2. For estimation of pharmacokinetic parameters, sample size varied over time with at least 13 participants (formulation 1) and at least 19 participants (formulation 2) due to early discontinuations for reasons unrelated to the study drug. Following administration of intramuscular lenacapavir, concentrations increased rapidly, and median time to maximum concentration was 84·1 days (IQR 56·1–112·0) for formulation 1 and 69·9 days (55·3–105·5) for formulation 2. The highest median concentration of once-yearly intramuscular lenacapavir (247·0 ng/mL [IQR 184·0–346·0] for formulation 1, 336·0 ng/mL [233·5–474·3] for formulation 2) remained above the highest median twice-yearly subcutaneous lenacapavir concentration (67·3 ng/mL [46·8–91·4]). Median Ctrough at the end of 52 weeks for formulation 1 was 57·0 ng/mL (IQR 49·9–72·4) and for formulation 2 was 65·6 ng/mL (41·8–87·1), exceeding the median twice-yearly subcutaneous lenacapavir Ctrough of 23·4 ng/mL (15·7–34·3) at the end of 26 weeks. Median AUCdays 1–365 for formulation 1 was 1011·1 h*μg/mL (IQR 881·0–1490·2) and for formulation 2 was 1274·0 h*μg/mL (1177·3–1704·8). Adverse events were mostly grade 1 or 2. The most common was injection-site pain (16 [80%] participants given formulation 1, 15 [75%] given formulation 2), which was generally mild, resolved within 1 week, and was substantially reduced by pretreatment with ice.
Interpretation
Following administration of once-yearly intramuscular lenacapavir, median plasma concentrations exceeded those associated with efficacy in phase 3 studies of twice-yearly subcutaneous lenacapavir for PrEP for at least 56 weeks. Both formulations were safe and well tolerated. These data show the potential for biomedical HIV prevention with a once-yearly dosing interval.
Additional documents
No documents were uploaded
Useful links
Collaborate for development
Consider on a case by case basis, collaborating on developing long acting products with potential significant public health impact, especially for low- and middle-income countries (LMICs), utilising the referred to long-acting technology
Share technical information for match-making assessment
Provide necessary technical information to a potential partner, under confidentiality agreement, to enable preliminary assessment of whether specific medicines of public health importance in LMICs might be compatible with the referred to long-acting technology to achieve a public health benefit
Work with MPP to expand access in LMICs
In the event that a product using the referred to long-acting technology is successfully developed, the technology IP holder(s) will work with the Medicines Patent Pool towards putting in place the most appropriate strategy for timely and affordable access in low and middle-income countries, including through licensing